Case history 05
Case history 05
Date of admission: 19-09-2021
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
50 year old female came to casuality with chief complaints of fever since 8days.
HISTORY OF PRESENT ILLNESS:
Patient was asymptomatic 8days back then she complaints of fever which is high grade associated with chills and generalized weakness.
Patient also complains of body pains and headache which relieved on medication.
Patient also complains of cough which is non- productive with food and water content which is not associated with shortness of breath.
Patient has a history of hysterectomy
No history of hematuria and rashes on the body.
No history of burning micturition.
PAST HISTORY:
Patient is a known case of diabetes mellitus, patient is on Tab Glimepride 1mg, Tab metformin 500mg.
There is no history of hypertension, Tuberculosis and asthma.
TREATMENT HISTORY:
patient had not undergone any treatment prior.
No history of chemotherapy and radiation.
No history of surgery.
FAMILY HISTORY:
There is a history of diabetes mellitus in the family.
GENERAL EXAMINATION:
patient is conscious, coherent and cooperative and well oriented to time, place and person.
No pallor, cyanosis, clubbing and generalized lympadenopathy.
VITALS:
SYSTEMIC EXAMINATION
RESPIRATORY SYSTEM:
•NVBS heard
•Position of trachea - central
•Breath sounds - vesicular
CENTRAL NERVOUS SYSTEM:
•Intact
•No focal defect
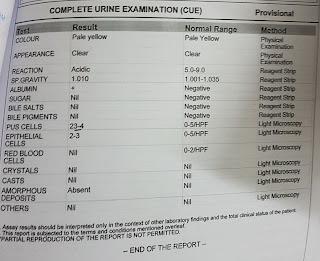
INVESTIGATIONS













Comments
Post a Comment